Defensive Charting For Nurses Course
Defensive Charting For Nurses Course - The concepts of skilled, reasonable, and necessary will be articulated in terms nurses and therapists will understand. List three problem areas in nursing documentation. One tool especially suited for defensive documentation is the acronym fact, which stands for factual, accurate, complete, and timely. The purpose of this module is to provide an overview of nursing documentation, outlining the professional standards, most common documentation errors, and legal risks of incomplete nursing documentation amidst evolving technology and reliance on electronic medical records. This defense is built carefully, meticulously, with detailed paper trails beginning from the moment the nurse first sees a patient. Describe documentation strategies for challenging situations. Step into the realm of comprehensive charting with advocate maggie for an unparalleled perspective. It also helps nurses meet standards of professional practice. The main thing is to stick to the facts only the facts, don't offer your own thoughts on things or try to write a story. Armed with a fundamental understanding of this information, clinicians will be able to meet documentation expectations. In this course, you will also understand documenting phone calls, the legalities of charting, and. Avoid value judgments, bias, labels, and subjective opinions. When documenting, record only information and behavior you observe. At its core, documentation should provide a nurse with an indisputable defense against malpractice. This course is designed to give learners an overview of the best documentation practices for anyone in healthcare who contributes to a client’s medical record. The main thing is to stick to the facts only the facts, don't offer your own thoughts on things or try to write a story. Describe two documentation strategies to reduce liability exposure. You’ll leave this course with a broader understanding of what effective charting looks like, as well as ineffective charting. Understanding and utilizing best practice of accurate defensive documentation will help avoid allegations of misconduct by way of misinformation. Armed with a fundamental understanding of this information, clinicians will be able to meet documentation expectations. This training course is intended to cover the knowledge and principles of good record keeping. The course will examine real examples of patient care and use lessons learned to vastly improve incident reporting and. What is required for nursing documentation? Cynthia will share her knowledge of how documentation is used in the legal arena with examples of common documentation pitfalls.. Armed with a fundamental understanding of this information, clinicians will be able to meet documentation expectations. Learn to chart like your license depends on it! Describe documentation strategies for challenging situations. The main thing is to stick to the facts only the facts, don't offer your own thoughts on things or try to write a story. One tool especially suited. In this course, you will also understand documenting phone calls, the legalities of charting, and. The main thing is to stick to the facts only the facts, don't offer your own thoughts on things or try to write a story. List three problem areas in nursing documentation. When documenting, record only information and behavior you observe. It also helps nurses. This defense is built carefully, meticulously, with detailed paper trails beginning from the moment the nurse first sees a patient. Cynthia will share her knowledge of how documentation is used in the legal arena with examples of common documentation pitfalls. The main thing is to stick to the facts only the facts, don't offer your own thoughts on things or. The purpose of this module is to provide an overview of nursing documentation, outlining the professional standards, most common documentation errors, and legal risks of incomplete nursing documentation amidst evolving technology and reliance on electronic medical records. Describe two documentation strategies to reduce liability exposure. When documenting, record only information and behavior you observe. The importance of creating a clearly. What is required for nursing documentation? This defense is built carefully, meticulously, with detailed paper trails beginning from the moment the nurse first sees a patient. For example, to meet standards related to evaluating a patient’s progress towards goals, the nurse and others on the healthcare team need to review past documentation. When documentation becomes your defense; This training course. Describe two documentation strategies to reduce liability exposure. This defense is built carefully, meticulously, with detailed paper trails beginning from the moment the nurse first sees a patient. It also helps nurses meet standards of professional practice. For example, to meet standards related to evaluating a patient’s progress towards goals, the nurse and others on the healthcare team need to. Describe documentation strategies for challenging situations. You’ll leave this course with a broader understanding of what effective charting looks like, as well as ineffective charting. Examples of good and bad charting; This class will engage both experienced and n ewer nurses. Understanding and utilizing best practice of accurate defensive documentation will help avoid allegations of misconduct by way of misinformation. In this course, you will also understand documenting phone calls, the legalities of charting, and. Compare and contrast documentation formats. For example, to meet standards related to evaluating a patient’s progress towards goals, the nurse and others on the healthcare team need to review past documentation. The main thing is to stick to the facts only the facts, don't offer. For example, to meet standards related to evaluating a patient’s progress towards goals, the nurse and others on the healthcare team need to review past documentation. Demonstrate nurses’ contribution to patient care outcomes. The main thing is to stick to the facts only the facts, don't offer your own thoughts on things or try to write a story. Cynthia will. This course will take you through the daily charting and documentation that is necessary for your patients. List three problem areas in nursing documentation. Describe documentation strategies for challenging situations. What is required for nursing documentation? Tips for passing medicare audits, charting incident reports and writing physicians’ orders accurately will all be discussed. When documenting, record only information and behavior you observe. Chart any procedures you do and patient response, chart pain and pain meds. The purpose of this module is to provide an overview of nursing documentation, outlining the professional standards, most common documentation errors, and legal risks of incomplete nursing documentation amidst evolving technology and reliance on electronic medical records. At its core, documentation should provide a nurse with an indisputable defense against malpractice. Avoid value judgments, bias, labels, and subjective opinions. This course is designed to give learners an overview of the best documentation practices for anyone in healthcare who contributes to a client’s medical record. Demonstrate nurses’ contribution to patient care outcomes. ~ legal lingo ~ general documentation tips ~ narrative note writing ~ incident report writing ~ crisis standards of care This course will update nurses on the requirements of medical record documentation as well as professional, responsible documentation strategies. Here is some information that can assist with improving your charting and reducing liability risks: This training course is intended to cover the knowledge and principles of good record keeping.Defensive Practice PDF Nursing Health Care

NCLEX Tip Defense Mechanisms Nurse study notes, Nursing school
Charting Cheat Sheet, Great for Nursing Students and New Grads Etsy

Defensive Documentation YouTube
Documentation

Defensive Documentation Practice For Nurses Capricorn Healthcare
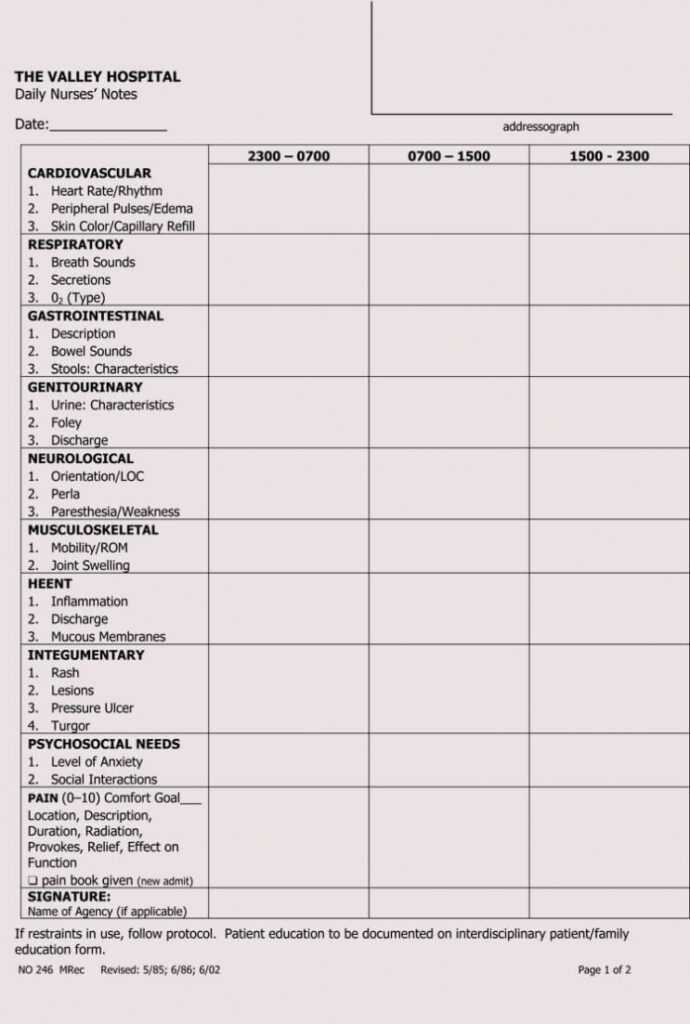
Nursing Assistant Report Sheet Templates

10 Charting in Nursing Dos and Don'ts CareerStaff Unlimited
Guidelines for Charting and Documenting Joyce University of Nursing

Defensive Documentation Practice For Nurses Capricorn Healthcare
The Main Thing Is To Stick To The Facts Only The Facts, Don't Offer Your Own Thoughts On Things Or Try To Write A Story.
In This Course, You Will Also Understand Documenting Phone Calls, The Legalities Of Charting, And.
When Documentation Becomes Your Defense;
Describe Two Documentation Strategies To Reduce Liability Exposure.
Related Post:
